Behavioral Ultrasound- child dental x ray
child
dental x ray On or around April
1, 1980, someone decided the objective of an ultrasound exam was a set of
images. It seems plausible on the surface. It fits the job description of
ultrasound technologists, and it mirrors the role of manufacturers. From the
standpoint of medical diagnosis, though, that notion departs from medical
teachings going back to Hippocrates, probably even earlier to the Ebers
Papyrus. I am sure the originator could
not have been a radiology. I hope
that behavioral psychology might provide
us with an insight.

In the Beginning
The early B-Mode
ultrasound settlement included physicians with a wide array of specialty
backgrounds. After some initial, and very significant, technical advances, a
lot of the daily clinical work across the country was handled by
radiologists. Along the way, cardiologists
moved up to high-speed imaging from TM tracings and obstetricians began to
offer ultrasound to their own patients. Now, we have separate ultrasonic
fiefdoms in multiple areas – the ER, the ICU, MSK, family, medicine, and, at
the recent AIUM, there were multiple presentations and courses on dermatologic
applications.
The early days were
a simple time. There wasn’t much known,
you didn’t have to know much, and clinical expectations were low. Acquiring
satisfactory images took a long time, and they had a low yield of actionable information.
The only impetus for clinical usage seemed to be avoiding ionizing radiation
exposure. Most of the uses revolved around distinguishing “cysts” from “solids”
for finding fluid collections of one type or another, or for looking at
movements of structures in a fluid field.
I think of the
decade from 1975 as the golden (and radiologic) Age of Ultrasound. There was a
vast amount of academic research of imaging fundamentals leading to some major
improvements in instrumentation, and there was a gigantic deepening of clinical
sophistication with a rich peer-reviewed literature. There were some massive technical downsides.
Image noise content was so high and data acquisition so varied from
place-to-place, from operator-to-operator, and between multiple types of
instruments that there was never any effective way to establish practice
standards, make education uniform, or extract quantitative descriptors of
tissue properties.
Nevertheless, the
clinical results of the early experience with mechanical and electronic
scanners were very good, and the field flourished over a wide span of
diagnostic applications. An essential factor may have been due to the way
radiologists handle visual data. The starting points for all imaging modalities
are knowing where to look and how to look. The real work is in fitting
information from images with everything you know clinically about the patient
and everything you should know about what can go wrong with that patient’s population cohort. The “list” of possibilities is prioritized by
the potential lethality or severity of probable conditions. The radiologist has
to have an understanding of the utility of every other diagnostic procedure in
his or her own facility in order to select the safest and most informative way
of resolving a clinical question as a procedural sequence.
Another covert facet
of image interpretation is the ability to extrapolate the consequences of a
diagnosis. This might seem obvious in a fetal or pediatric ultrasound study,
but it is always a factor. Perhaps this is why radiologists have been so
obsessed with the pick-up rates, the sensitivity, and the specificity of
screening exams ever since the days of mobile vans for tuberculosis detection.
If you miss a tiny, eminently miss-able, lesion, the patient might lose years
of life. Over-diagnosis has its own set of painful and costly detriments.
Fast and/or Slow
My limited exposure
to “dual process theory” is from Thinking, Fast and Slow by Daniel Kahneman
(Farrar, Strauss, Giroux, 2011 ISBN: 978-0374275631). This book has been
referred to as a masterpiece. It has won every possible award. It explored the
life work of the author and his late collaborator Amos Tversky, and it centers
on “prospect theory” – the basis for Professor Kahneman’s Nobel Prize in
Economics. The subject is treated scientifically. It describes many ingenious
experiments, which established there are two main ways people respond to
situations, referred to as “fast” and “slow.” The works of other researchers is
detailed selflessly, and there are no wild speculations. Since this work
concerns basic human behavior, it would seem logical that it applies to
ultrasound, too.
Fast and slow are
metaphors. The fast system is instant, automatic, unconscious, capricious,
effortless, and always on. It is triggered by unconscious perceptions and works
by ingrained associations and patterns that are very hard to change. It is
incapable of calculation. It is not influenced by statistics or objective
reality. It is gullible and can be misled. Effective ads appeal to the fast
system.
Slow is rational,
conscious, suspicious, and very effortful, because it involves a lot of energy
expenditure. Fast can be brilliant, but prone to systemic errors; slow can be
thorough and plodding, but it is not “perfect” either. Slow is mostly off, and
it can be derailed by emotionally-tainted fast perceptions, as well as a
limited knowledge base.
I’ve always believed
in love at first sight. That is an ultimate fast system response. Fast is very
efficient, and it works by a system of heuristics. “Heuristics” is a relatively new word, coined
from a Greek root related to discovery, so its definition remains somewhat
pliable. I encountered the term in college (it’s probably common in grade
schools now) in issues related to computer searching, pattern recognition, and
artificial intelligence. An heuristic is a fast, efficient, down-and-dirty
shortcut for getting a workable and/or reasonable, approximate solution to a
complex, sometimes analytically insoluble, problem. In Thinking, Professor
Kahneman identifies several classes of heuristic that the fast system relies
upon. One is the “halo effect” in which your impression becomes generalized
over the object, i.e. love at first sight = everything about the object of your
affections is lovable and perfect. Heuristics are mental habits. It is also via
heuristics that biases emerge as influencers.
A Detour to
Psychiatry and Genetics
Fast has been
proposed as the evolutionary default state. Each of us has a balance point
between fast and slow in our lives and work that I want to explore a little
more. People who are locked into either of these operational states exclusively
have well defined forms of psychopathology. People with very different balances
between fast and slow cannot communicate very well. People who are mainly fast
double down on their opinions, even when they have no factual substance or
foundation, and mainly slow people cannot understand the emotional fervor of
preferential fasts. All of my patients are referred, and to tell you the truth,
I have always found a lot of remote referral patterns to be somewhere between
rigid and irrational. I would guess these referrals are fast responses by
practitioners who don’t know a lot about ultrasound, don’t keep up with
technical advances in the field, and often resist informed suggestions about
effective utilization of resources.
Let’s start with the
common expression “Crazy runs in families.” This is true, but it has been very
difficult to clarify because a family tree peppered with psychoses has so much
variability by type, severity, and age of onset that their occurrence can seem
random or at least unrelated. Genome
sequencing has identified multiple loci for a spectrum of psychoses in which
the specific whose combination of genes, and their penetrance seem to explain
those variations. At one end of the
spectrum is potential brilliance, the other hallucinatory divorce from reality.
Think of the phrase: “She’s as pigheaded as her father.” Doesn’t it seem likely
that the balance between fast and slow is also coded into our genomes?
Postgraduate Medical
Education
How has medicine
coped traditionally with these unrecognized fast/slow issues? Take a bunch of
young people with good hearts and stellar academic records. They have
altruistic heuristics, learn well, and adapt to variability and chaos. This is
an ideal, new medical school class. They receive a progressive increase in information
over several years to nourish their slow systems. But, there is even more
emphasis on interactive topics, like taking a history. This can be viewed as a
way to mold the fast system for dealing, bonding, and gaining the trust of new
patients despite first impressions on both sides. It also creates an indelible
bond with our professional ancestors who have all had to cope with the same
issue.
Medical specialty
training expands upon integrating the two systems in some way. I look back in
awe, admiration, and fondness to my time as a diagnostic radiology house
officer at the Massachusetts General Hospital (MGH). I was probably not so
sanguine at the time. I presume the educational goals of all diagnostic
radiology training programs are identical everywhere. I have never had any need
to inquire of colleagues about their own background, because of the
similarities of our perceptions and work habits.
Reading plane films
started out as a slow system endeavor. You try to look at every detail of all
of the views you have before you. It’s very tiring, exhausting, actually, and
that’s before you even start to integrate clinical information and narrow down
diagnostic possibilities. You keep hearing phrases like, “get the Gestalt”
without knowing what that means until, magically, you get it. There are
withering comments for errors, in public at conferences and more privately when
reviewing a board full of cases. There is scarcely anything positive for a good
call. It is much milder than the surgical experience. The system is geared
toward emergent decision making and directed towards avoiding errors, and if an
error is made, to be sure that it is not repeated.
The only way to
handle a large volume of imaging studies efficiently is by identifying any
anomalies in any part of a film at a glance. The slow system does not get
evoked unless the fast system signals it needs to be activated. To do that
effectively, the fast system has to be able to cope with all kind of films,
with technical factors, including artefacts, and with a full range of normal
variations. The immediate correlates are anatomical; the inferences are
pathophysiological.
Plainly,
radiologists are marvelous, especially at radiology. Every specialist has gone
through a similar kind of education in their own fields, but because so much of
fast system training is not conscious,
you cannot relate to alternate ways of instant processing in other
disciplines, even if they all share scientific foundations. You may know the end result of someone’s
clinical work, but not the way he or she got there.
There has been a
progressive ultrasound procedure drain from radiology into other fields that
have not had the years it takes for fast
system retraining for medical visual information work. It can succeed, but
usually for specific questions with simple yes and no kinds of answers. It
obviates the general diagnostic utility inherent in the method and the nature
of its form of tissue mapping. The fast
system response of an unfortunate number of radiology departments to turf
issues seems to have been to relegate ultrasound to the cabinet of curiosities
and to move on in other imaging directions.
Interpreting Outside
the Box
Articles about
ultrasound without images are like desserts without carbs. If you’re like me
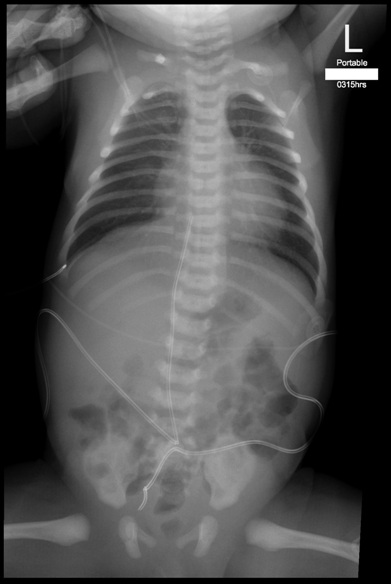
you’ve already looked at the image. See anything interesting?
I selected an image
from a recent visit to a level III NICU. Among ultrasound’s advantages is that
high resolution, high contrast imaging can be performed in the isolette without
disturbing the endlessly fragile and vulnerable small premie. Studies tend to
be on demand when there is a suspicion of a problem. There are often no
baseline views for comparison or pre-emptive screening for early diagnosis.
The renal image was
from a female premie identified as a “normal” control, without any other
information provided. For the time being, go with this one view and assume
there were similar appearances for a few other papillae on both sides, but
nothing else. The fast system says:
yellow alert, something unusual and unexpected, presumptively pathological.
There is also a vibe that the problem is local and that its cause may have been
a drug side effect. The slow system cannot
go much further without a lot more information, starting with why this child
was delivered early and whether there may have been hydramnios. Then, it
will want ALL of the available clinical information, and it may want to review
what is known about renal pathology in newborns. Are the image findings
predictive of nephrocalcinosis or
predispose to papillary necrosis? Or will the appearance revert to normal with
the accelerated healing of fetuses and newborns? There is not any available
data to know the significance of the finding for renal development in early childhood
treatement or function in adolescence and adulthood. There is a nice review of high resolution
ultrasound of the pyramids which raises the same concerns by A Daneman et al,
Renal Pyramids: Focused Sonosgraphy of Normal and Pathyologic Processes in
Radiographics.
Prospect Theory
One of the main
research areas of Thinking has to do with how people make investments. What
struck me was the framing of the concept with a strong condition of “loss aversion.”
The first aphorism of Hippocrates states something like: Whatever you do, don’t
make things worse. Radiology has the operative dicta: Do not miss anything in
an image. Do not fail to provide information to contribute to a therapeutic
action plan. We are all really risk and loss aversive.
Kahneman and Tversky
found people faced with the same test problems may act to gamble one time and
not to another, depending on the way the problem is phrased, as well as their
moods and biases at the time. In addition, investors decided to “go for it” or “back off,” depending on
assessments of luck and expectation of rewards. This is the fast system at work
– biased, not quantitative. In our routine work, the equivalent might be the
way an exam is conducted for a happy situation like a normal pregnancy with a
goal of wellness confirmation versus the bleak scenario of staging an invasive
carcinoma or searching for metastases. Very busy work schedules, limited
patient contact time, and overly focused exam goals, promote reliance on
habitual fast thinking.


Comments
Post a Comment